
Alisha Alderson placed her folded clothes and everything she needed for the last month of her pregnancy in various suitcases. She never imagined she would have to leave the comfort of her home in rural eastern Oregon just weeks before her due date. But following the abrupt closure in August of the only maternity ward within 40 miles, she decided to stay at her brother’s house near Boise, Idaho — a two-hour drive through a mountain pass — to be closer to a hospital.
“We don’t feel safe being so far away from a birthing center,” said Alderson, noting her advanced maternal age of 45. “I was sitting in a hair salon a few days ago and some people started joking about me giving birth on the side of the road. And in that moment, I just pictured all the things that could go wrong with my baby and broke down in tears in front of strangers.”
A growing number of rural hospitals have been shuttering their labor and delivery units, forcing pregnant women to travel longer distances for care or face giving birth in an emergency room. Fewer than half of rural hospitals now have maternity units, prompting government officials and families to scramble for answers.
One solution gaining ground across the U.S. is freestanding midwife-led birth centers, but those also often rely on nearby hospitals when serious complications arise.
The closures have worsened so-called “maternity care deserts" — counties with no hospitals or birth centers that offer obstetric care and no OB providers. More than two million women of childbearing age live in such areas, the majority of which are rural.
Ultimately, doctors and researchers say, having fewer hospital maternity units makes having babies less safe. One study showed rural residents have a 9% greater probability of facing life-threatening complications or even death from pregnancy and birth compared to those in urban areas — and having less access to care plays a part.
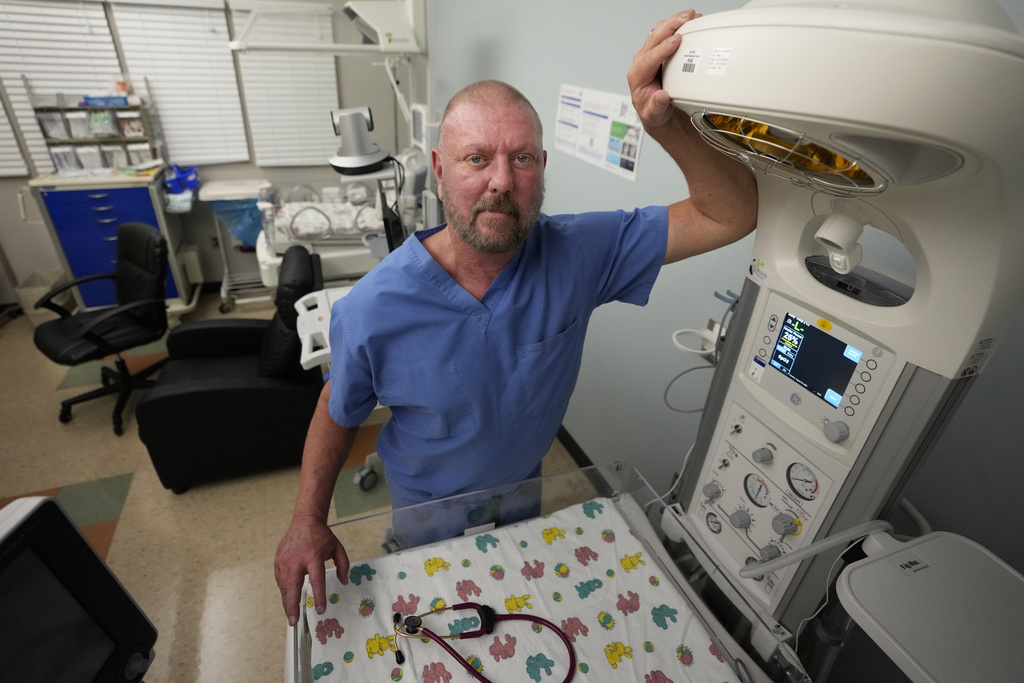
“Moms have complications everywhere. Babies have complications everywhere,” said Dr. Eric Scott Palmer, a neonatologist who practiced at Henry County Medical Center in rural Tennessee before it ended obstetric services this month. “There will be people hurt. It’s not a question of if — simply when.”
Reasons behind the closures
The issue has been building for years: The American Hospital Association says at least 89 obstetric units closed in rural hospitals between 2015 and 2019. More have shuttered since.
The main reasons for closures are decreasing numbers of births; staffing issues; low reimbursement from Medicaid, the federal-state health insurance program for low-income people; and financial distress, said Peiyin Hung, deputy director of the University of South Carolina’s Rural and Minority Health Research Center and co-author of research based on a survey of hospitals.
Officials at Saint Alphonsus, the hospital in Baker City where Alderson wanted to give birth, cited a shortage of OB nurses and declining deliveries.
“The results are devastating when safe staffing is not provided. And we will not sacrifice patient safety,” according to an emailed statement from Odette Bolano and Dina Ellwanger, two leaders from the hospital and the health system that owns it.
While they said financial concerns didn’t factor into the decision, they underlined that the unit had operated in the red over the last 10 years.

A lack of money was the major reason why Henry County Medical Center in Paris, Tennessee, closed its OB unit. CEO John Tucker told The Associated Press that it was a necessary financial step to save the hospital, which has been struggling for a decade.
The percentage of births there covered by Medicaid — 70% — far exceeded the national average of 42%. Tennessee’s Medicaid program paid the hospital about $1,700 per delivery for each mom, a fraction of what the hospital needed, Tucker said.
Private insurance pays hospitals more — the median topped $16,000 for cesarean sections in Oregon in 2021. State data shows that’s more than five times what Medicaid doles out.
Tucker also said the number of deliveries had dropped in recent years.
“When volumes go down, losses actually get bigger because so much of that cost is really fixed,” he said. “Whether we’ve got one baby on the floor or three, we still staff at the same level because you kind of have to be prepared for whatever comes in.”
The last week in a delivery ward
Six days before the Tennessee unit closed, just one woman was there to deliver. All of the other rooms contained empty beds and bassinets. The special care nursery was silent — no beeping machines or infants’ cries. Art had been removed from the walls.
Lacy Kee, who was visiting the ward, said she’ll have to drive 45 minutes and cross the state line into Kentucky to give birth to her third child in early October. She’s especially concerned because she has gestational diabetes and recently had a scare with her fetus’ heart rate.
Kee also had to switch from the Henry County obstetrician she trusted for her other pregnancies, Dr. Pamela Evans, who will stay at the hospital as a gynecologist.
Evans fears that things like preterm deliveries, infant mortality and low-birthweight babies — a measure in which the county already ranks poorly — are bound to get worse. Prenatal care suffers when people must travel long distances or take lots of time off work for appointments, she said. Not all insurance covers deliveries out of state, and some alternative in-state hospitals families are looking at are an hour or more away.
Evans' office and exam rooms contain bulletin boards covered with photos of infants she’s brought into the world. During a recent visit, Katie O’Brien of Paris handed her a new photo of her son Bennett — the third of her children Evans delivered. The two women cradled the baby and hugged.
The closure “makes me absolutely want to cry,” said O’Brien, 31. “It’s a horrible thing for our community. Any young person looking to move here won’t want to come. Why would you want to come somewhere where you can’t have a baby safely?”
A place to turn
About two hours away, inside a house in the woods, a handful of women sat in a circle on pillows for a prenatal group meeting at The Farm Midwifery Center, a storied place in Summertown, Tennessee, that's more than a half-century old.
Led by midwife Corina Fitch, the women shared thoughts and concerns, and at one point tied on scarves and danced together. One by one, Fitch pulled them into a bedroom to measure bellies, take blood, listen to fetal heartbeats and ask about things like nutrition.
Betsy Baarspul of Nashville said she had an emergency C-section in a hospital for her first child. She’s now pregnant with her third, and described the difference between hospital care and birth center care as “night and day.”
“This is the perfect place for me,” she said. “It feels like you’re held in a way.”
Some states and communities are taking steps to create more freestanding birth centers. Connecticut Gov. Ned Lamont recently signed legislation that will license such centers and allow them to operate as an alternative for low-risk pregnancies.
Alecia McGregor, who studies health policy and politics at the Harvard T.H. Chan School of Public Health, called midwife-led birth centers “a major sort of contender among the possible solutions” to the maternity care crisis.
“The kinds of lifesaving procedures that can only be conducted in a hospital are important for those very high-risk cases,” McGregor said. “But for the majority of pregnancies, which are low-risk, birth centers can be a very important solution to lowering costs within the U.S. health care system and improving outcomes.”
A lack of data and the small number of births in freestanding centers or homes prevents researchers from fully understanding the relationship between birth settings and maternal deaths or severe injuries and complications, according to a 2020 report from the National Academies of Sciences, Engineering, and Medicine.
The Farm said fewer than 2% of clients end up having C-sections, and a report on deliveries in its first 40 years showed 5% of clients were transported to the hospital — which Fitch said can happen because of things like water breaking early or exhaustion during labor. Clients usually give birth at The Farm or in their own homes.
“We always have a backup plan," she said, “because we know birth is unpredictable and things can come up.”
Rural hospitals will need to be part of the equation, doctors told the AP, and they believe governments must do more to solve the maternal care crisis.
Oregon politicians mobilized when the Baker City hospital announced in June that it was shutting down its birth center — including Oregon Gov. Tina Kotek, U.S. Sen. Ron Wyden and Baker County Commissioner Shane Alderson, Alisha's husband. As a temporary fix, they suggested using OB nurses from the U.S. Public Health Service Commissioned Corps, a branch of the country’s uniformed services that largely responds to natural disasters and disease outbreaks.
It was a novel and “innovative” idea to request federal nurses to boost staffing at a rural maternity unit, Wyden’s office said. While it didn’t end up panning out, the public health service sent experts to Baker City to assess the situation and recommend solutions — including looking into establishing a freestanding birth center.
Shane Alderson wants to help people who are facing the same tough decisions his family had to make. He said rural communities shouldn’t be stripped of health care options because of their smaller size or because of the number of low-income people with public insurance.
“That’s not equitable,” he said. “People can’t survive like that.”

___
Rush reported from Baker City, Oregon, and Kuna, Idaho. Ungar reported from Paris, Tennessee, and Summertown, Tennessee.
___
The Associated Press Health and Science Department receives support from the Howard Hughes Medical Institute’s Science and Educational Media Group and the Robert Wood Johnson Foundation. The AP is solely responsible for all content.